
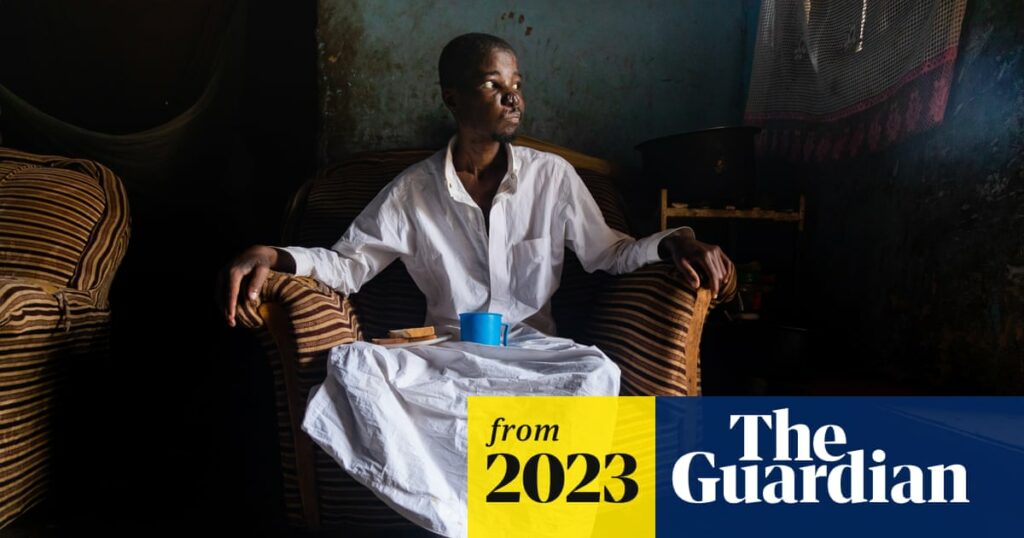
Alex Mubiru shuffles out of the bare-brick bedroom that he shares with his brother and two nephews. Weakened by Aids and cancer, he spends his days lying on a thin mattress in the dark, but nurse Roselight Katusabe is here to check on him so he is helped by his girlfriend, Florence, into the cramped front room of his mother’s house in Wakiso village.
Since he was diagnosed in October with Kaposi’s sarcoma, a type of skin cancer that is common in people who are HIV positive, Mubiru’s health has deteriorated rapidly. Katusabe is concerned that his laboured breathing could be a sign the cancer has spread to his lungs, but the family can barely afford food, let alone £200 for the tests needed for him to start chemotherapy at the Uganda Cancer Institute, about 15km away in the capital, Kampala. The crops that his mother planted to provide for the family were stolen in December. Mubiru, a 31-year-old father of three, says simply: “I want to go to work again.”
Without treatment, the prognosis for Mubiru is not good. Katusabe does her best to ease his pain, giving him morphine and antibiotics for an infection, and a package with maize flour, beans, rice and sugar. As well as providing vital nutrition, the food means he can take antiretrovirals for HIV without severe side-effects.
Alex Mubiru at home with his mother, Aida Nakakande. Without money for chemotherapy, nurses at Hospice Africa Uganda provide him with pain relief and food
Mubiru’s situation is typical of the cases that Katusabe and her colleagues at Hospice Africa Uganda (HAU) deal with on a daily basis – and it indicates the huge challenge facing the pioneering palliative care organisation.
About 70% of the 2,000 patients on HAU’s programme have cancer, and some are HIV positive, too. Few can afford tests or treatment for their conditions and, even when they can, it is not uncommon for doctors to misdiagnose or fail to prescribe adequate pain relief. Often, by the time a patient is referred to HAU, their condition is incurable, much to the frustration of the team, whose goal is to offer palliative care from the moment a person is diagnosed with a life-limiting condition.
Nurse Roselight Katusabe (centre) talks to Aida Nakakande about what can be done to help Mubiru, while his girlfriend, Florence Nalugoti, waits outside
“One of our biggest challenges is to remove the stigma [around palliative care]. Some people think it is about dying, but it is for anyone with a chronic illness that is not going away,” says Antonia Kamate Tukundane, programmes manager at HAU’s Mbarara site in south-west Uganda. “Palliative care focuses on holistic care: How are you? How is your family? What other things are affecting your illness? We provide something the doctors and nurses have no time for.
Dr Anne Merriman at home in Kampala. She founded Hospice Africa Uganda in 1993, with a vision to introduce “palliative care for all in need in Africa”
“Sometimes the patient comes to us very ill and passes on, but if we had known the patient earlier we could have explained what was happening to their body; agreed on realistic goals; all this is so helpful for the patient. Those who find us are glad they did.”
HAU was founded in 1993 by Irish doctor Anne Merriman, who still lives in Kampala, though, at 87, has stepped back from the day-to-day running of the organisation. Today, HAU is run by a team of just over 70 health professionals and admin staff across three city sites: Kampala, Mbarara and Hoima in the west, and is a model for palliative care not just in Uganda, but across Africa.
In 1993, HAU became the first organisation to introduce oral liquid morphine into Uganda after persuading the government the risk of addiction was extremely low. Dr Merriman, who had developed a formula while working in Singapore, made it herself “at the sink with a bucket”. “It’s as easy as making coffee, just four ingredients: morphine powder, a preservative, PH stabiliser and water. And it’s cheap too,” she says.
A sign divides a cancer ward at Mbarara hospital into male and female patient areas
At the time, only three countries in Africa allowed access to the medication – Zimbabwe, Kenya and South Africa – compared with 37 today. HAU takes some credit for this thanks to its international programme that offers training and placements for champions of palliative care across the continent.
Lack of morphine
In 2004, the government passed legislation that made HAU the sole producer of liquid oral morphine in Uganda, to be distributed by the National Medical Stores and prescribed for free by nurses. Previously only doctors and dentists were allowed to prescribe it but with only one doctor per 50,000 people at that time it was vital that nurses were trained to use it too.
Today, the medication is mixed by a machine donated by the American Cancer Society, but the small facility at HAU’s Kampala site still produces only a fraction of what is needed. According to the Palliative Care Association of Uganda (PCAU), every year just 11% of the estimated 500,000 Ugandans needing palliative care, including pain relief, have access to it. This compares well with many low-income countries, where levels of avoidable pain are even worse.
Liquid oral morphine is produced for distribution by the National Medical Stores at HAU’s facility in Kampala, Uganda
A 2018 Lancet report on global palliative care described lack of morphine as “a heinous injustice that has been largely ignored in global health”.
“Of the 298.5m metric tonnes of morphine-equivalent opioids distributed in the world each year, only 0.1 metric tonnes are distributed to low-income countries, and 50% of the global population (3.6 billion people residing in the poorest countries) receive less than 1% of the morphine distributed worldwide,” it said.
Nevertheless, Uganda has not progressed at the rate experts hoped for. “Uganda has stagnated,” says Dr Emmanuel Luyirika, executive director of the African Palliative Care Association (APCA). “Though the government has done a fantastic job on access to oral morphine, in terms of overall funding of health, it has not done well.”
Health spending in Uganda is just 2.3% of GDP, well below the 15% agreed by African governments in 2001. The result is a health system ill-equipped to meet the universal health care goals, where hospitals are desperately understaffed, the poor cannot access treatment and the rich travel abroad in search of cures.
Sarah Nabushawo, head nurse at Mbarara hospital’s oncology department, where she is the only government-paid nurse
At the oncology department in Mbarara hospital, Sarah Nabushawo is the only government-paid nurse overseeing the patients. “It is very stressful,” she says. “Patients expect you to work on time but we only have one oncologist.”
Quality of life
Outside Mbarara hospital, every day, up to 100 people wait on wooden beaches to be assessed. Those who are eventually seen are screened by a junior doctor in a cramped room where it is impossible to talk in private. The seriously ill and those in need of chemotherapy and blood transfusions stay on the ward, where patients often have to sleep on the floor. On the paediatric ward there are up to three children to a bed.
skip past newsletter promotion
Sign up to Global Dispatch
Get a different world view with a roundup of the best news, features and pictures, curated by our global development team
Privacy Notice: Newsletters may contain info about charities, online ads, and content funded by outside parties. For more information see our Privacy Policy. We use Google reCaptcha to protect our website and the Google Privacy Policy and Terms of Service apply.
after newsletter promotion
A lack of state funding means not only that frontline services are stretched but also that the government cannot fulfil its commitment to palliative care. A palliative team established by the health ministry in 2022 to oversee the integration of palliative care into the health system has no dedicated budget.
Cancer patients wait to be seen at Mbarara hospital
Nurses and doctors who gain a qualification at the Institute of Hospice and Palliative Care Africa (IHPCA), the education arm of HUA, end up returning to their former roles because there is no budget for specialist ones.
“At least 226 health facilities offer a form of palliative care,” says Mark Mwesiga, executive director of PCAU. “But they are offering it as an added role and we would like the government to recognise, recruit, remunerate and retain people as palliative care providers.”
Before I couldn’t sleep day or night, I would lie and listen to my pain. But now I think about other thingsBeinomugisha Ephraim
Dr Muwanga Moses, assistant commissioner in charge of medical services at the health ministry, acknowledges that “resources are limited”, but suggests lack of palliative care in hospitals is a structural rather than economic failure. “It is up to the hospital to create the right structure to create jobs and manage the budget.”
The government has also stalled on legislation. A palliative care policy to create a framework for national standards, including paid roles in hospitals, has been in draft form for five years. “Since we started five years ago, the person in charge has changed three times,” says Luyirika. “Uganda has dragged its feet.”
Legislation would also boost awareness of palliative care at all levels, from potential patients to community leaders and medical professionals. “Most of our patients have gone ‘doctor shopping’ in different areas,” says Katusabe. “They are desperate to find a cure – and at some point they find someone motivated by money; they go to herbalists or spiritual leaders who are not telling the truth. When they come to us, they have spent all their money. They don’t have food and can’t afford basic medication.”
As the burden of non-communicable diseases increases, so, too, does the need for palliative care. The Uganda Institute of Cancer in Kampala, the only facility in the country that offers radiotherapy, is seeing up to 6,000 new cases a year, according to consultant haematologist Dr Henry Ddungu. “It is the tip of the iceberg. Less than 20% of cancer patients come to the institute. Of those who do, over 80% have either stage three or four of the disease – and they all qualify for intense palliative care.”
Dr Henry Ddungu, consultant haematologist at the Uganda Institute of Cancer in Kampala
Dr Ddungu would like to see a specialised palliative unit at the cancer institute. Until that happens, it continues to refer patients to HAU. But drastic cuts in funding have left HAU’s already tight resources even more stretched. In the past decade, its income has halved from 7.5bn Ugandan shillings a year in 2012 to 3bn in 2022, leading to a steep drop in staff and a reduction in home and hospital visits. Weekly drop-in sessions that gave families, including children, some relief from their caring duties now run monthly.
Much of the money came from Aids programmes that stopped funding palliative care when more people with HIV started taking antiretrovirals. Today, international aid is heavily weighted towards preventive and measurable activities. Palliative care – with softer outcomes, such as restoring independence, dignity and relieving anguish – is a harder sell to donors.
Lead nurse Martha Rabwoni walks through a banana plantation on her way to visit a patient about 15km outside of Mbarara
Depleted funds mean every member of staff at HAU is a multitasker. At Mobile Hospice Mbarara, lead nurse and health services coordinator Martha Rabwoni gets ready to visit 60-year-old Beinomugisha Ephraim, who has Aids and late-stage cancer. The last time she visited, she had to supervise the construction of a bed after a colleague reported he had been left lying on the dirt floor.
Reaching the remote house involves a 15km drive, the last part along a dusty red track followed by a walk through a banana planation, but Rabwoni is pleased to find Ephraim sitting up in bed smiling. She has brought him fresh sheets, soap, food, and morphine. He tells her he is on better form: “Before, I couldn’t sleep day or night. I was so cold. I would lie and listen to my pain, but now I think about other things.”
But Rabwoni is concerned that the family is not capable of looking after Ephraim. They are barely surviving on the pittance the daughter-in-law earns working for nearby farms. “Palliative care is about so many other things. You do what you think needs to be done,” she says, making a note to tell the local council the family has no latrine and no kitchen – basic requirements it is responsible for monitoring even in the most remote communities.
Martha Rabwoni, head nurse at Mobile Hospice Mbarara, attends to Beinomugisha Ephraim, who has Aids and late-stage cancer
When her colleague checks in on Ephraim a few days later, he is still in good spirits and tells them stories. But the next morning they receive a call to say that he died that night.
Back in Kampala, Katusabe returns to see Mubiru. “After the nutrition, he has some energy, and now he can walk from the house to the compound,” she says. HAU has funded some of the tests he needs, but not all, and he still hasn’t begun the life-saving cancer treatment. In the meantime, Katusabe will keep giving the practical and psychological support her limited budget allows.
“In palliative care we don’t give up,” she says. “There is always something we can do.”
Source link : https://www.theguardian.com/global-development/2023/mar/06/ugandas-pioneers-of-palliative-care-undaunted-by-huge-challenges-acc
Author :
Publish date : 2023-03-06 08:00:00
Copyright for syndicated content belongs to the linked Source.