Our model supports the notion that a complex interplay between different drivers determines the timing and speed of the transition from a concentrated to a generalized HIV epidemic across different countries and sub-regions. In Madagascar, we believe that two major factors may have been modulating disease expansion, and delaying this potential transition: the late/slow introduction of HIV and/or widespread practice of circumcision [15]. According to our analyses, HIV prevalence should have been very low still in 2000 according to the earliest data available from 2005 [20] and 2007 [21], but estimated R0 was already much larger than 1 in most cities. Therefore, the model reveals that the protective effect of circumcision was minimal back then, and may have already vanished in Madagascar (Fig. 3). This is in agreement with previous authors, which pointed out that over certain threshold of HIV prevalence among sex workers, circumcision does not have a substantial effect towards HIV prevention at population level [22]. Furthermore, our results suggest that the turning point towards generalized epidemic in Madagascar is very close or may have even been surpassed in certain localities (Fig. 4). At this stage, AGYW may play a key role mediated by transactional sex in the generalization and maintenance of the epidemics in the general population (Fig. 6), with a key interaction with acute HIV infections.
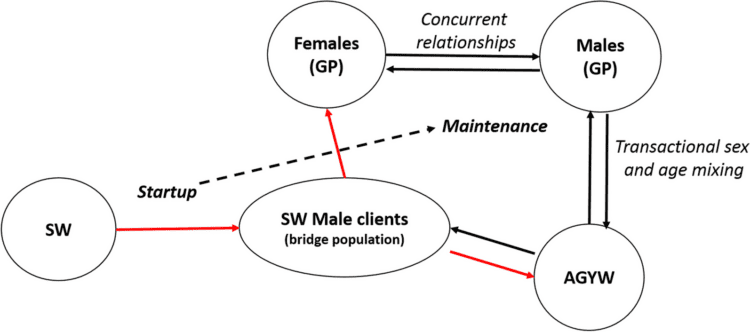
Fig. 6
Conceptual model of HIV progression from concentrated epidemic to generalized and self-maintained epidemic in countries with the socio-behavioural characteristics of Madagascar. The start up of the epidemic is characterized by a long-lasting and steady increase of HIV prevalence among SWs. HIV infection spills over to GP (adult females, AGYW and indirectly other GP males) through bridge population (SW clients, see red arrows). The intensity of this initial spillover is enhanced as prevalence among SW increases in a positive feedback manner. Once a certain threshold in GP has been reached, prevalence/incidence in GP may be self-sustained and tend to increase through high risk intercourse between AGYW and older adults. This threshold may be reached sooner depending on the prevalence of age disparate relationships, concurrency and inconsistent use of condoms. Transactional sex may be the main mediator of such risk factors. SW sex workers, GP general population, AGYW adolescent girls and young women
However, the generalization of the HIV epidemic is far from a homogeneous process across the 11 studied cities, and it looks more like a patchwork of micro-epidemics leading to different regional and subregional stages (Fig. 2). In spite of this heterogeneity, according to our model future HIV prevalence in Madagascar for next decade (2030s) may be similar to other HIV/AIDS highly hit countries from the Southern African region between 9 and 24%, unless a sustained action is taken.
Our model is based on the key recognition of commercial sex as the main driver of HIV infection leading to a generalized epidemic in Sub-Saharan Africa [22]. However, we expanded the classical concept of sex workers, encompassing the consideration of transactional sex (occasional sexual intercourse in exchange of any material or non-material benefit other than money). Transactional sex has been underscored as a risky factor for HIV expansion [23], and it is especially prevalent among AGYW and well documented in Madagascar [2, 24]. A disproportionate fraction of sexual encounters between males and younger females (intercourse mixing age heterogeneity, factored by the parameter fW and f0, see Additional file 1: Table SB1 and SB2, and also Fig SE7), has been early noticed as a risk factor of HIV acquisition for AGYW on itself, and through associated risky behaviors, such as concurrency and inconsistent use of condoms [25,26,27]. Thereby, AGYW is now considered as a truly key population in most Sub-Saharan countries [5], with six or sevenfold higher risk of HIV acquisition compared to males of the same age [27, 28]. In Madagascar, all of these factors and behaviors have been reported as highly prevalent [2]. Of note, the widespread presence of sex working and transactional sex is strongly influenced by underlying socio-economic factors, such as financial insecurity and poverty [27] and structural factors such violence and criminalization [29]. Consequently, our model may underestimate the speed of transition towards generalized epidemics if a major economic crisis occurs, as we expect as consequence of epidemic outbreaks like COVID-19 or climate change impacts in form of droughts and secondary food insecurity, as it has been recently experienced in Madagascar [30], which may in turn hamper the HIV response [31]. Indeed, it has been underlined the disproportionate susceptibility of women to these factors [32]. For this reason, it is striking to observe that future projections about the impact of these crisis on HIV/AIDS epidemic, focus almost entirely on the effect on the sustained provision of anti-retroviral drugs and HIV-services [33, 34] without considering the indirect impact on the economy and other cofactors.
In agreement with previous work [35, 36], our model predicts that the sex workers population is the first to take off in the trajectory towards disease establishment (Fig. 5a). At that point, sex workers HIV prevalence may be the startup of the HIV introduction into the general population through bridge populations (clients), followed by a further expansion of HIV infection mediated by transactional sex mainly practiced by AGYW and older males. Therefore, the intercourse mixing-age model and risky behaviors associated to transactional sex may play a crucial role in the spread and maintenance of the epidemics once HIV prevalence has reached a certain threshold among general population (see Fig. 6). At a certain stage, the HIV epidemics evolve independently from the number of HIV positive sex workers [35]. The inclusion of different infectiousness levels (see Fig. 1) through the stages of the natural history of a HIV infection allows to explore their interaction with behavioral factors which are particularly associated to the described pattern of sexual encounters [37], and circumcision. Here, we strongly suggest that acute infections would play an important role in the epidemics transition. Accordingly, previous authors pointed out the disproportionate contribution of acute infections at the early stages of disease expansion [38]. Although most previous HIV compartmental models of this kind [39, 40] do not consider these critical interactions, previous work considering some of them leads to similar conclusions [36].
Main parameters of HIV transmission established by previous observational studies lie within the bounds of our model estimations. Scarce HIV cases has been reported in Madagascar at least since 1989 [41]. Therefore, we calculated R0 values in 2000, when prevalence was still thought to be very low. These values depend on most model parameters, and vary between about 3 and 9 across the different cities (Fig. 2) in good agreement with observational estimations [42]. However, these estimations may be a little inflated because they are calculated under the assumption of random sexual contacts between the different groups [43]. Notwithstanding, these values are particularly useful for relative comparisons, and to elucidate which model parameters have the highest influence on disease propagation just after HIV introduction. They represent highest bounds, as it is known that in general contact heterogeneity, and non-random sexual mixing (for instance, sequential monogamy), commonly slows down disease propagation [44]. In summary, from our case-study, we suggest that factors influencing the transition towards a generalized HIV epidemics result from a complex interplay between geographic isolation, which may be enhanced by political issues, slowing down the introduction of HIV, cultural practices, such as circumcision, but as well the societal consideration of women and gender-based practices that may protect young women from risky behaviors (i.e. early marriage, matriarchal structures), biological (i.e. the key role of acute infections during the transitional phase), and socio-economic disruptions. The transition from rural to urban societies, with the interaction between all these elements, may exacerbate these underlying factors (erosion of traditional practices, increasing population mobility and lack of social protection towards AGYW).
Our study is limited first by the scarce information available on the distribution of women in the different key groups (Sex-workers and transactional sex, and non-sex-workers or -transactional sex). Specific hypotheses controlling this distribution are implicitly assumed in the set of α and σ’s parameters (see Fig. 1 and Additional file 1: Tables SA1, SB1 and SB2). Second, there is no direct data on the age-disparity of sexual relationships in Madagascar, and finally, the paucity of epidemiological time-series data, as pointed out previously [2]. Furthermore, we do not considered other key populations (men who have sex with men and injected drug users), which have been largely neglected in Sub-saharan Africa [45], but their role in the generalization of epidemics should not be discarded. In fact, the role of injected drug users has been particularly underscored in Sub-Saharan Africa [46], and this represents an increasing population in Madagascar [2]. The bridge between these key population and the general population through bisexual intercourses and sex working, should be further explored. Future models of this kind should also take into account mobility between localities as pointed out recently [47, 48]. At this stage, our model does not consider the movement of populations at risk (specifically sex workers) between cities following tourist seasons, as it has been reported in Mahajanga and Nosy-be (the two cities with higher HIV prevalence among sex workers, Fig. 2) [2, 24]. These dynamics may foster even more diffusion of HIV to other parts of the country. For the seek of simplicity, we have not included Sexually Transmitted infections (STI), which increase the risk of HIV transmission and susceptibility [49], as well as schistosomiasis infection which is highly prevalent in Madagascar [50], and may contribute to the diffusion of HIV through their genital manifestations (Male and Female Genital Schistosomiasis) [51, 52]. Finally, we did not considered the impact of ARV coverage, which is already very low according to official reports [53] and, therefore, its current role in containing the diffusion of HIV is probably very limited.
Our projections should be considered a call for action given the scant attention that HIV in Madagascar has received, and the Public Health crisis that potentially could unfold, but could still be avoided. Furthermore, the lack of inclusion of coinfections (STI and schistosomiasis) and mobility between cities and a possible underestimation of the amount of AGYW practicing transactional sex could make our model projections still conservative.
Considering the discussed limitations, our model cannot be simply regarded as a predictive exercise and projections should be considered with caution. However, according to our results a generalized epidemics can not be ruled out under reasonable assumptions. In this sense, it is worrisome to see that Madagascar shows some of the poorest HIV response indicators in the world (only 14% of persons living with HIV are estimated to be under follow-up and this data was not considered in our modeling estimates) [53]. Given the plausibility of the worst case scenario outlined in this article, it is important to set up observational studies on HIV prevalence/incidence and risky factors that would help to draft more accurate predictions, alongside the implementation of robust preventive measures focused on monitoring and identifying hot-spots and vulnerable key populations (sex workers and AGYW). Finally, the case-study of Madagascar can help to understand how has occurred (or may occur) the transition from concentrated to generalized epidemics in different settings.
Source link : https://idpjournal.biomedcentral.com/articles/10.1186/s40249-023-01164-2
Author :
Publish date : 2023-12-07 08:00:00
Copyright for syndicated content belongs to the linked Source.


{kind=link}