If Cabo Verde can remain diligent, the country will be eligible to apply for malaria elimination certification in early 2021. Here, was described the malaria cases reported in Cabo Verde over the previous 10 years to characterize the transition to successfully eliminating transmission. This work highlights two, non-mutually exclusive challenges for elimination countries to sustain their gains: the risk of epidemics and continued importation. Reported locally acquired malaria cases prior to the 2017 epidemic were generally low, ranging from 0 to 30 cases per month and the estimated R0 being less than 1 for most years. In contrast, infections have been consistently imported into Cabo Verde and are reported in almost all municipalities. Understanding these trends, where and when imported infections are most likely to occur, and their potential to lead to onward transmission will be essential to sustain elimination and avoid future malaria epidemics.
To achieve malaria elimination in Cabo Verde, there has been a strong political commitment and investment in the health system [20,21,22]: there is good coverage of the health system across the country and is freely accessible to all residents. Malaria has been considered a notifiable disease for some time, to ensure that all cases are confirmed, offered supervised treatment with an effective antimalarial drug, and investigated within 24 h of reporting. Although information on individuals suspected and tested for malaria would strengthen confidence that all infections are identified, the data available for this analysis was largely complete with few missing data points. The investment to ensure complete, high-quality surveillance data will enable evidence-based targeting of resources and rapid responses to eliminate and monitor for any future epidemics [23]. Similarly, as part of strengthening the surveillance system, intensive training on classifying imported infections is essential to ensure local transmission is adequately measured. Effective classification and recording of the likely origin of infection also provides crucial information as to if and where intervention activities can be targeted to those individuals and/or areas most at risk [24,25,26,27]. Although the majority of infections were identified in males, this variable was not retained in the adjusted analysis. This is likely due to the limited heterogeneity for detecting associations. However, the results suggest that the frequent travel from Cabo Verde to endemic countries in continental Africa and being an adult under 40 years of age appears be the most important risk for re-introduction of malaria, putting the island’s malaria-free status at risk in the future [28, 29].
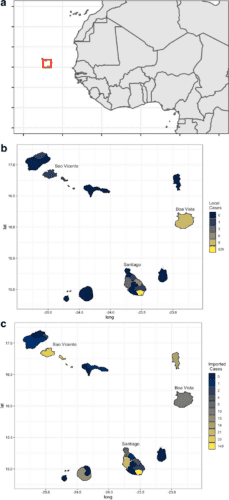
From the data over the ten years examined in this analysis, the capital city, Praia, experienced the highest burden of malaria cases in the country, including locally acquired (largely driven by the epidemic), imported, and also the two introduced infections. Praia is the largest urban area in the country, has the highest population of people traveling, including nationals and immigrant workers, and has frequent flight connections to endemic countries [28, 30]. Combined with the presence of semi-permanent breeding sites, which allow the persistence of Anopheles arabiensis in several neighbourhoods of the city, conditions in the city are highly conducive to malaria transmission [31,32,33]. Maintaining accessibility to health facilities, clinical management capacity for malaria and continued vector control will be important factors to prevent reestablishment of malaria transmission in the city, as well as other municipalities with a high degree of importation.
There are some limitations to this analysis to note. Firstly, the data available was obtained as part of routine surveillance. Although individual level case data from 2010 was available with few missing records, the breadth of potential covariates was limited thereby precluding more in depth analysis. Also, several variables were included in the regression modelling that serve as proxies. For example, although the population size was correlated with island, it improved the model fit and likely serves as a proxy for the probability of a case being identified. Similarly, epidemic period and year are also correlated. Despite the correlation and attempted alternative modelling forms (i.e. interactions), one of the variables may be acting as a proxy for changes in the surveillance system or malaria control program or shifts in how importated infections were classified. Finally, this data analysis was conducted with data collected as part of the routine malaria surveillance system. Therefore, not all potential covariables were available for analysis and the uneven distribution of indigeneous and imported infections across the islands and over time may have reduced statistical power to detect meaningful differences as is observed in the wide confidence intervals. Despite these limitations, the results are nevertheless informative.
Source link : https://malariajournal.biomedcentral.com/articles/10.1186/s12936-020-03455-7
Author :
Publish date : 2020-10-23 07:00:00
Copyright for syndicated content belongs to the linked Source.


{kind=link}